Thank you

COLON
Prof. Kang-Moon LEE
Prof. Seong Woo JEON
Prof. Stepan SUCHANEK

CASE 1
CASE 2
CASE 3
How do I use PENTAX IMAGINA in my clinical endoscopy cases :
“ I use PENTAX IMAGINA for colorectal cancer surveillance in patients with long-standing ulcerative colitis (UC).
Previously, I had performed surveillance using traditional random biopsies or pan-chromoendoscopy with targeted biopsies,
which required a lot of effort and time. Recently, however, I’m using image-enhanced endoscopy (virtual chromoendoscopy)
like NBI or i-scan which is more convenient.
Although still controversial, high definition-virtual chromoendoscopy is known to be comparable to dye-spraying chromoendoscopy in detecting neoplasia in UC.
I assume that combination of high-definition endoscopy with i-scan of PENTAX IMAGINA system can be useful for colorectal cancer surveillance in UC.“
Neoplasia Surveillance in Ulcerative Colitis with i-scan
Patient History
A 51-year-old male patient with long-standing ulcerative colitis underwent surveillance colonoscopy for detection of dysplasia.
Endoscopic Findings
With HD-WLE, old cicatricial changes with whitish scars and numerous inflammatory polyps were observed throughout the entire colon distal to A-colon. There showed no active lesions. (image 1)
With HD + i-scan, an ovoid flat elevated lesion (6 mm) was detected in mid T-colon. The lesion showed brown and irregular. Surface. (image 2)
Another ovoid flat lesion (4 mm) was detected in proximal T-colon. (image 3)
i-scan helped to find dysplasia and demarcate the borders of the lesions.
Endoscopic Treatment and Pathology Results
Two lesions were removed by endoscopic mucosal resection.
he final pathology was ‘tubular adenoma with low grade dysplasia’ in both lesions.
Patient Outcome and Follow-ups
Two colitic neoplasia were detected and removed successfully by surveillance colonoscopy.
The patient recommended to have regular surveillance colonoscopy.
Image 1
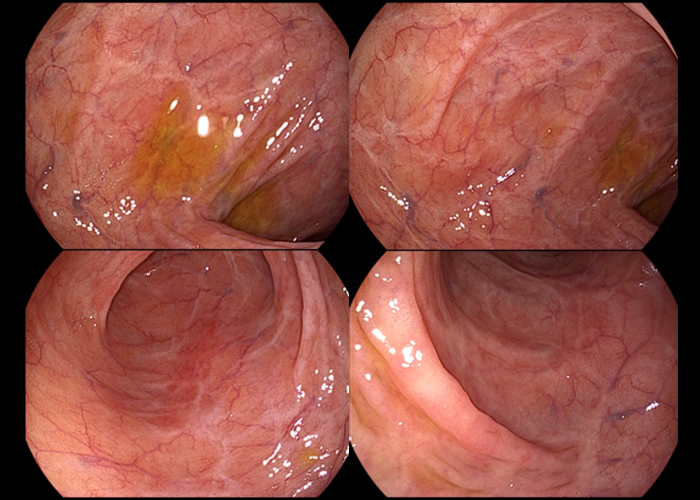
Image 2
Image 3
Summary

How do I use PENTAX IMAGINA in my clinical endoscopy cases :
“ I use PENTAX IMAGINA in my endoscopic procedures.
When an endoscopist performs a procedure, securing clean vision and smooth operation of endoscopy are essential factors. In this aspect, clear resolution and good maneuverability of PENTAX IMAGINA can be of great help to my successful procedure.”
Prophylactic Clip Application for the Prevention of
Postpolypectomy Bleeding of Large Pedunculated Colonic Polyps
Patient History
A 46-year-old male patient was referred for a large pedunculated colon polyp.
Endoscopic Findings
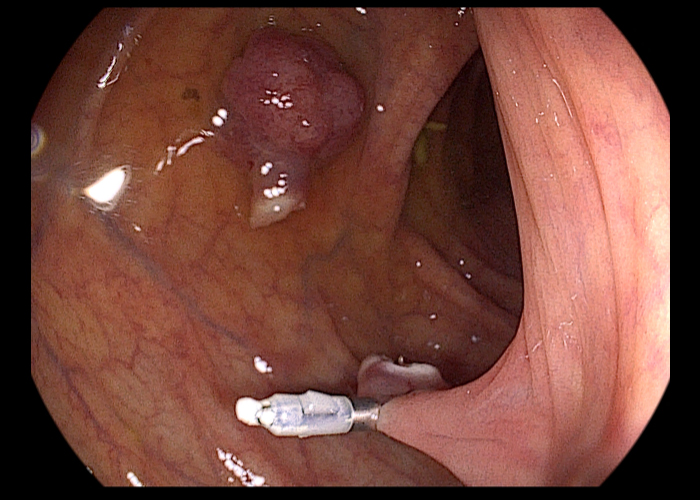
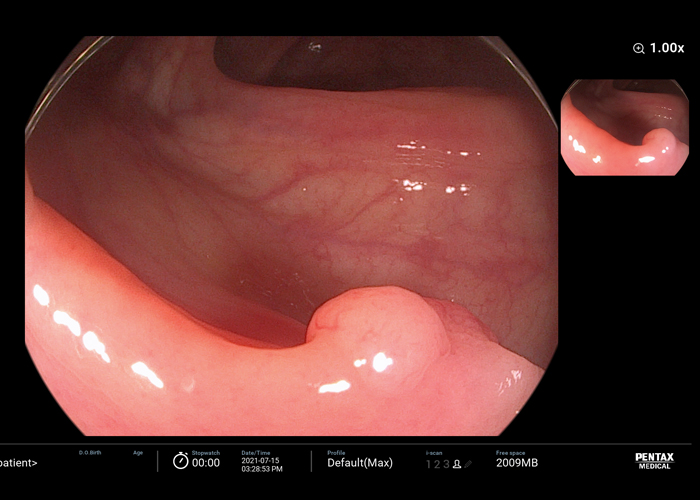
With HD-WLE, a 15 mm sized pedunculated polyp was noted in the hepatic flexure. The length and width of stalk was 30 x 8 mm. (image 1)
The surface of the polyp head showed hyperemia and nodularity.
With HD + i-scan, vessels with variable caliber and irregular surface pattern were noted. (image 2)
i-scan helped to define the microvascular and surface patten of the lesion.
Endoscopic Treatment and Pathology Results
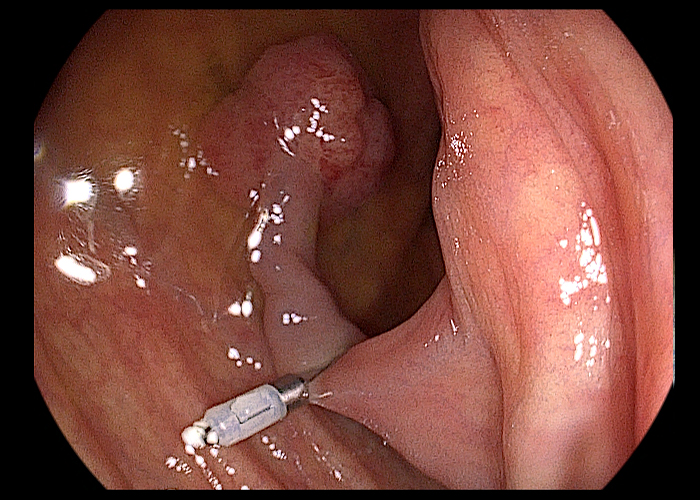
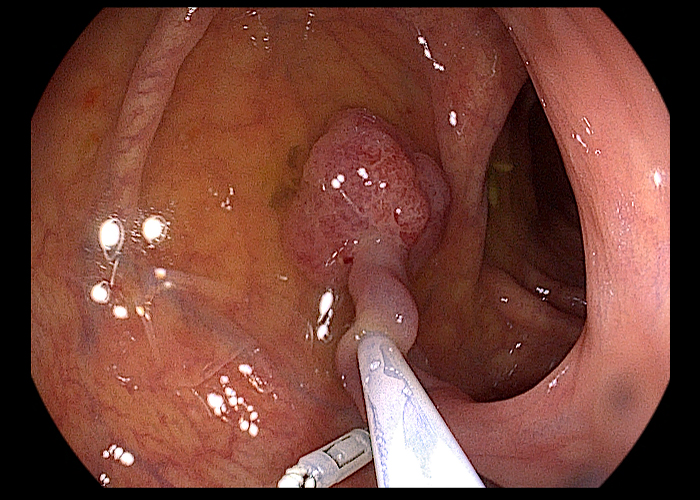
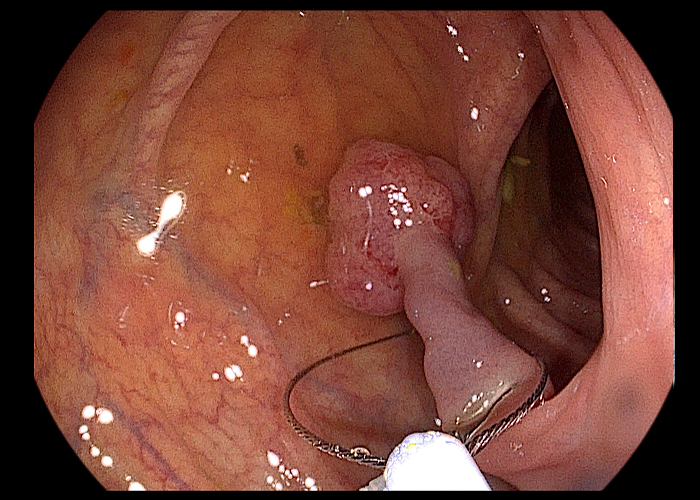
To prevent post-polypectomy bleeding, hemoclip was applied to the base of stalk before resection.
Then, hot snare polypectomy was performed. (image 3)
The final pathology was early colon cancer.
Adenocarcinoma, moderately differentiated, arising in sessile serrated adenoma with cytologic dysplasia
a) Size: adenoma 1.5 x 1.5 cm, carcinoma 0.7 x 0.7 cm
b) sm invasion = 300 ㎛ (Haggit level 1)
c) Tumor budding: absent
d) Resection margin involvement: absent
Image 1
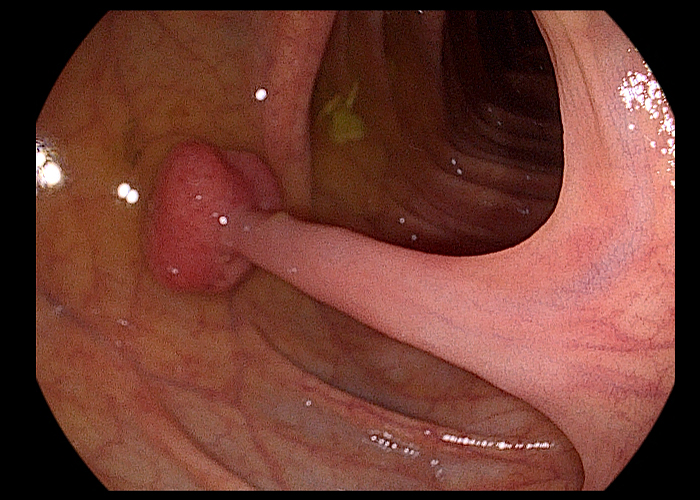
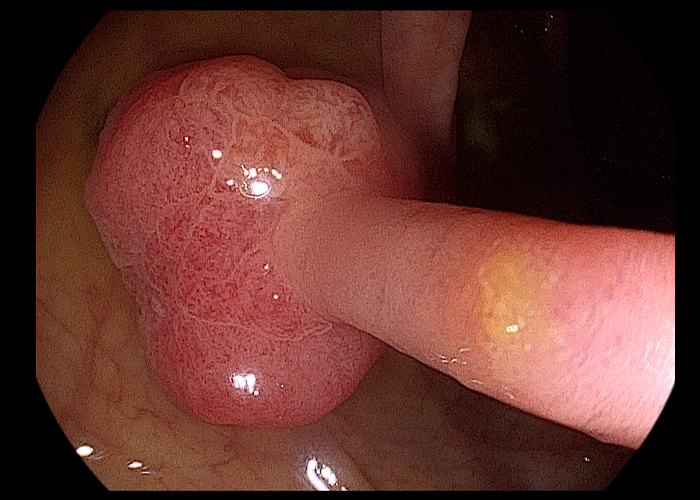
Image 2
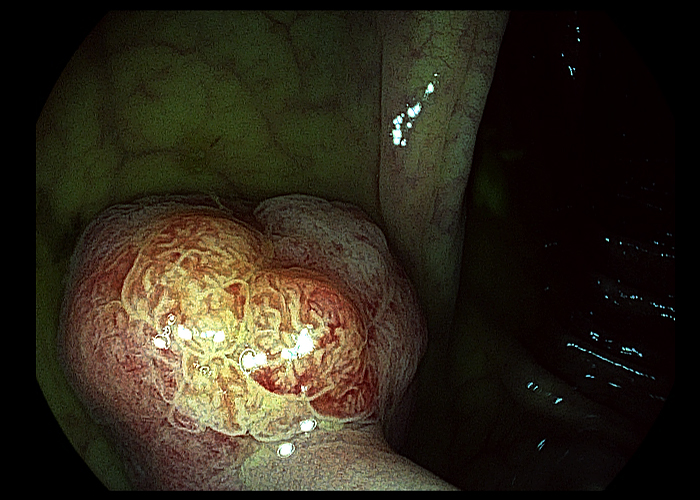

Image 3
Summary

How do I use PENTAX IMAGINA in my clinical endoscopy cases :
“ I use PETAX IMAGINA for colorectal cancer (CRC) screening. Higher quality colonoscopic withdrawal techniques, such as
(1)examining the proximal sides of flexures, folds and valves, (2) cleaning and suctioning, (3) adequacy of distention, and
(4) adequacy of time spent viewing, are associated with lower adenoma missing rate.
I think that clean resolution and good maneuverability of PENTAX IMAGINA may help to improve the yield of CRC screening.”
Detection of Sessile Serrated Adenoma in the Ascending Colon
Patient History
A 60-year-old female patient underwent colonoscopy for bloating and constipation.
Endoscopic Findings
With HD-WLE, a subtle flat lesion was suspected in the distal A-colon.
After adjusting for air inflation, an ovoid flat elevated lesion was clearly observed. (image 1)
With HD + i-scan, the surface of lesion showed slightly lighter color than background mucosa and some dark dots, suggesting a hyperplastic or
sessile serrated polyp. (image 2)
i-scan helped to define the microvascular and surface pattern of the lesion.
Endoscopic Treatment and Pathology Results
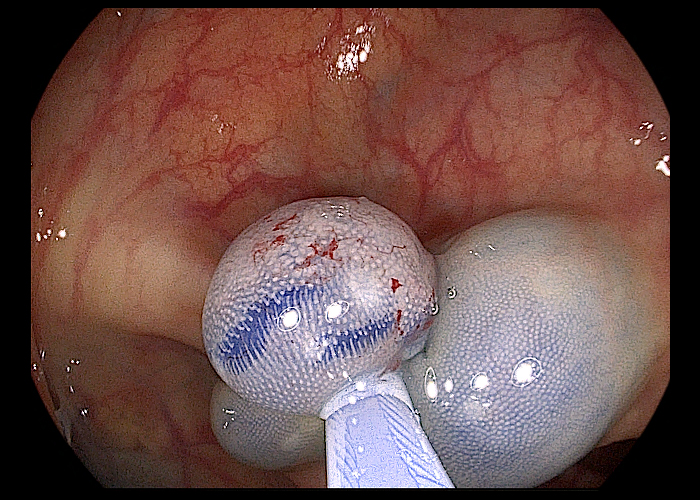
Endoscopic mucosal resection was done. (image 3)
The final pathology was sessile serrated adenoma.
Sessile serrated adenoma without cytologic dysplasia.
1) size: 0.8x0.8cm
2) resected margin involvement: absent
Patient Outcome and Follow-ups
The procedure performed successfully without any event.
Image 1
Image 2
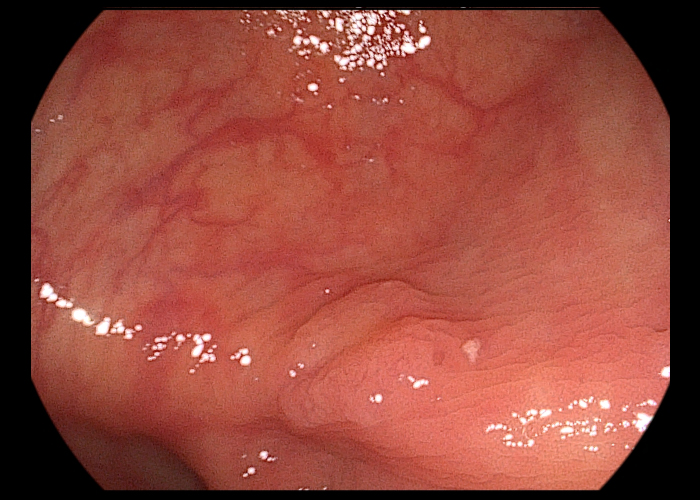
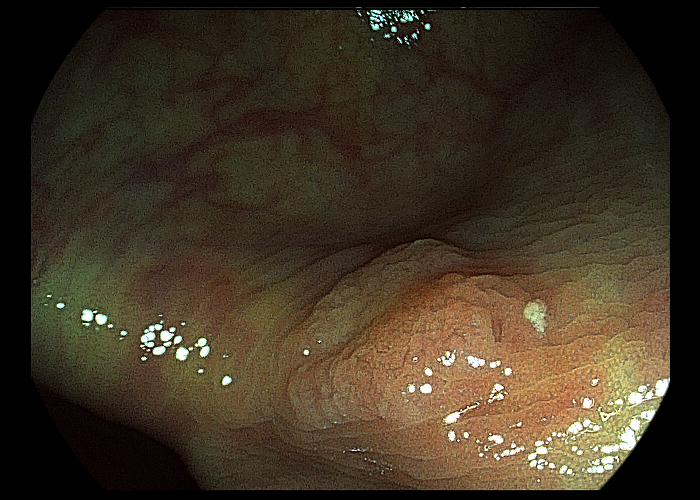
Image 3

Summary

COLON
Prof. Kang-Moon LEE
Prof. Seong Woo JEON
Prof. Stepan SUCHANEK
How do I use PENTAX IMAGINA in my clinical endoscopy cases :
“I use PENTAX IMAGINA in daily clinical endoscopy practice. One of our endoscopy purpose is surveillance after surgery or endoscopic resection of colorectal dysplasia or cancer. I frequently encounter metachronous polyps during this surveillance and the pathology provide exact diagnosis after resection of the polyp.
However, it is important to select exact candidates for colonoscopic resection to avoid unnecessary procedure.
I assume that PENTAX IMAGINA TE mode is useful in this aspect. JNET classification is useful tool in clinical decision.
Type 1 indicates a hyperplastic polyp or a sessile serrated adenoma/polyp.
Type 2A indicates low-grade dysplasia and includes tubular adenoma and tubulovillous adenoma.
Type 2B indicates high-grade dysplasia, intramucosal cancer, and superficial submucosal invasive cancer.
Type 3 indicates deep submucosal invasive cancer.
The PENTAX IMAGINA system have clear resolution and it can let me help to clear diagnosis. “
Endoscopic Differentiation of Colon Polyps
Patient History
The patient is a 61-year-old male who underwent sigmoid colon cancer surgery 2 years ago.
He is on adjuvant chemotherapy and colonoscopy surveillance was recently performed.
Endoscopic Findings
The colonoscopy revealed 8mm sized sessile polyp at transverse colon.
Endoscopic Treatment and Pathology Results
Endoscopic mucosal resection was done after submucosal injection and snaring.
No bleeding or perforation was noted after procedure. The final pathology was tubular adenoma, measuring 8mm in size.
Patient Outcome and Follow-ups
The patient will have another surveillance colonoscopy 2 or 3 year later.
Image 1,2 & 3
Video clip available
The i-scan SE shows sessile polyp with whitish surface mimicking sessile serrated polyp. However, the vascular and surface pattern was regular without white spots on i-scan TE image.
So, I can expect the pathology as a low-grade dysplasia based on JNET classification.
Summary

COLON
Prof. Kang-Moon LEE
Prof. Seong Woo JEON
Prof. Stepan SUCHANEK

CASE 1
CASE 2
How do I use PENTAX IMAGINA in my clinical endoscopy cases :
I use the IMAGINA system in every day clinical practice, especially in colorectal cancer screening program.
The high-quality image has resulted in an increased numbers of polyps detected.
Endoscopy mucosal resection of traditional serrated
lesion with high-grade dysplasia in sigmoid colon
Patient History
65 years old men with no CRC family history. Preventive colonoscopy after positive fecal immunochemical test.
Endoscopic Findings
Sessile polyp in aboral sigmoid colon (20 cm from anorectal line), Paris classification 0-Is, size 30 x 20 mm,
macroscopically adenomatous appearance according to the high-definition white light endoscopy
(HD-WLE, Image 1), i-scan 1 (Image 2), i-scan 2 (Image 3), i-scan 3 (Image 4)
Endoscopic treatment
Polyp was completely removed by endoscopic mucosal resection (EMR), after submucosal injection of saline solution with diluted Adrenaline.
Immediate bleeding from post-EMR site (Image 5) was stopped with snare tip coagulation, haemoclips and nylon loop snare replacement(Image 6).
Endoscopic Treatment and Pathology Results
Traditional serrated lesion with high-grade dysplasia, R0 resection.
Patient Outcome and Follow-ups
No sign of bleeding recurrence. Surveillance colonoscopy in 1 year negative with intact scar and no metachronous lesions in colorectum.
Image 1
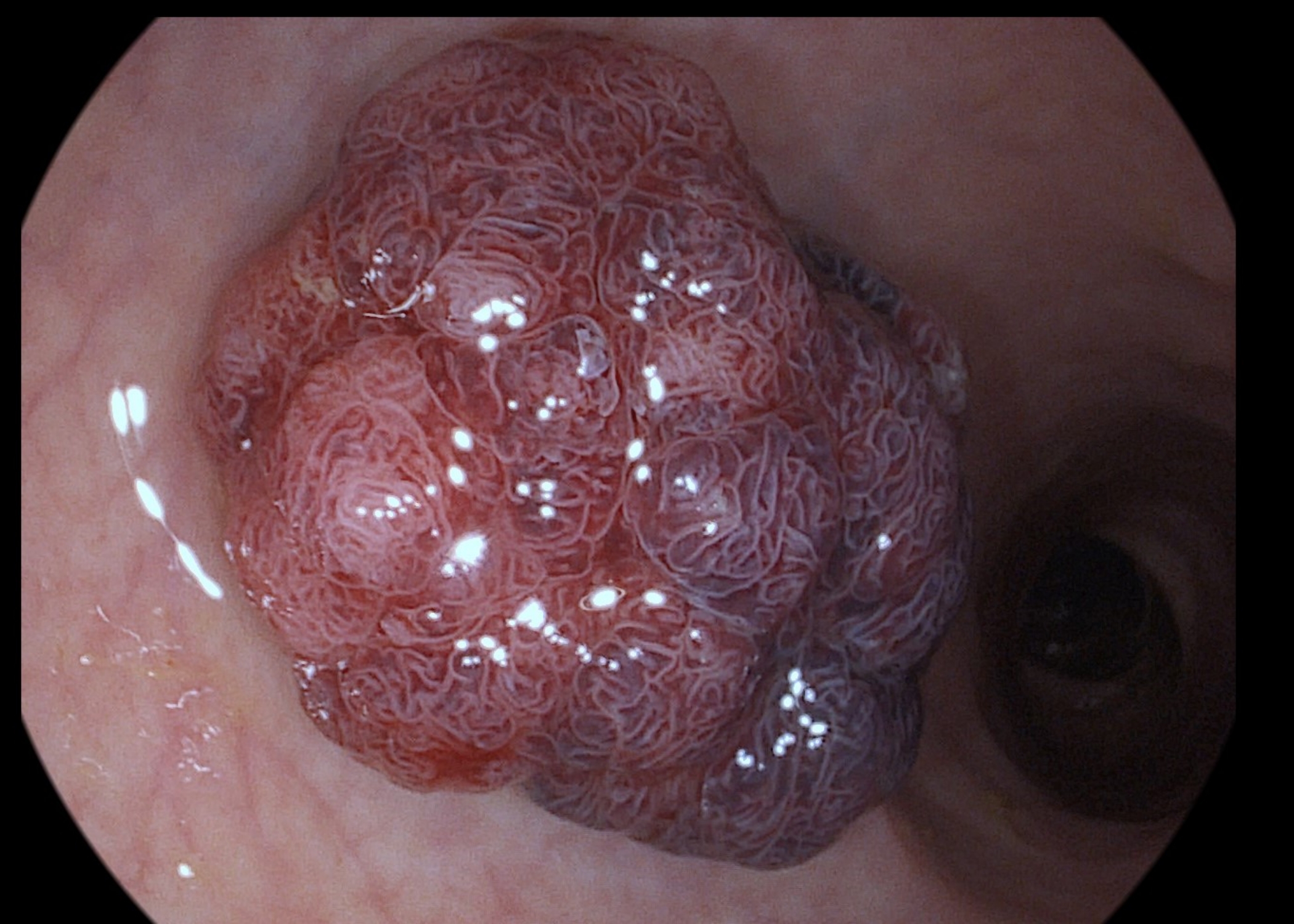
Image 2
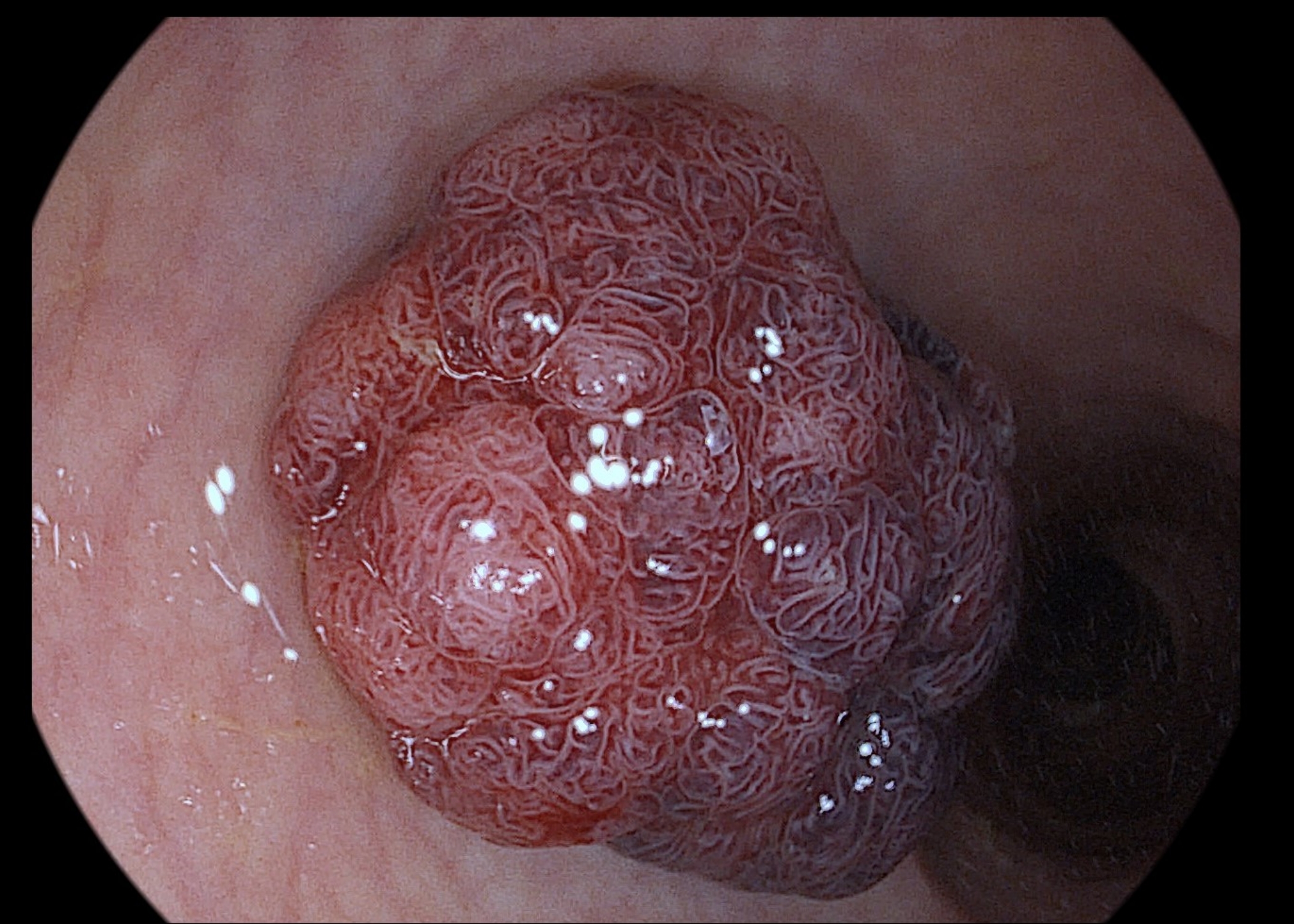
Image 3
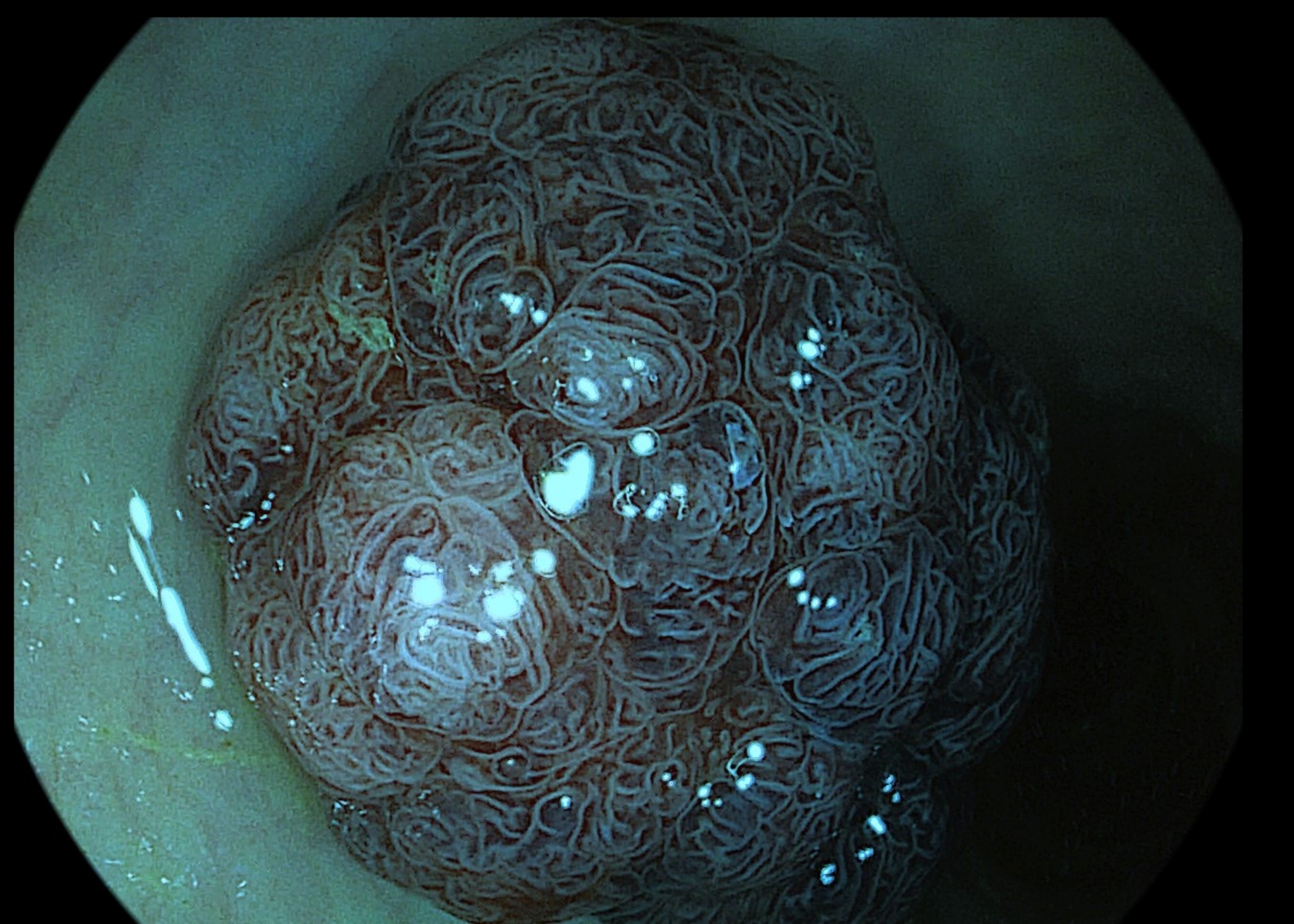
Image 4
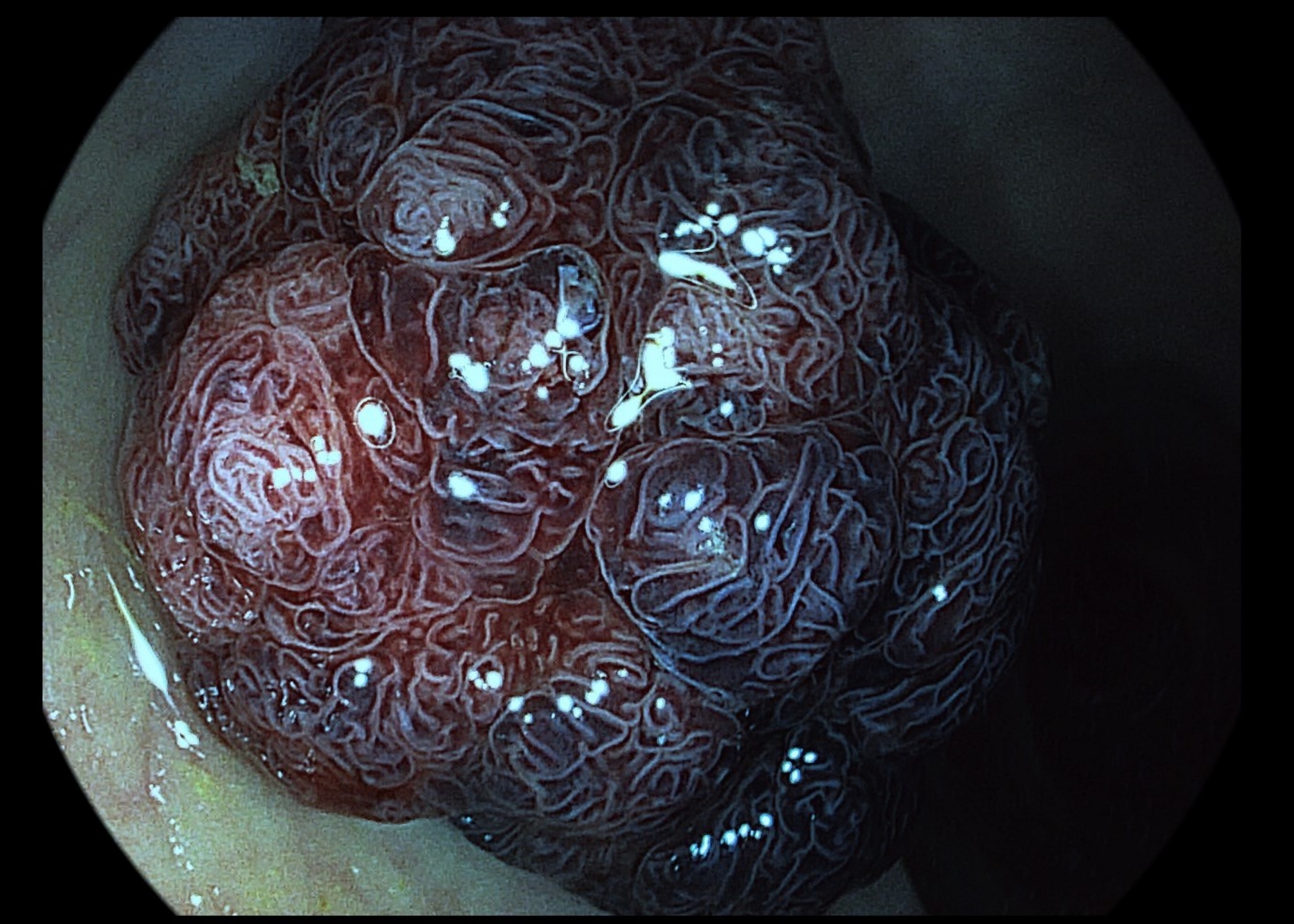
Image 5
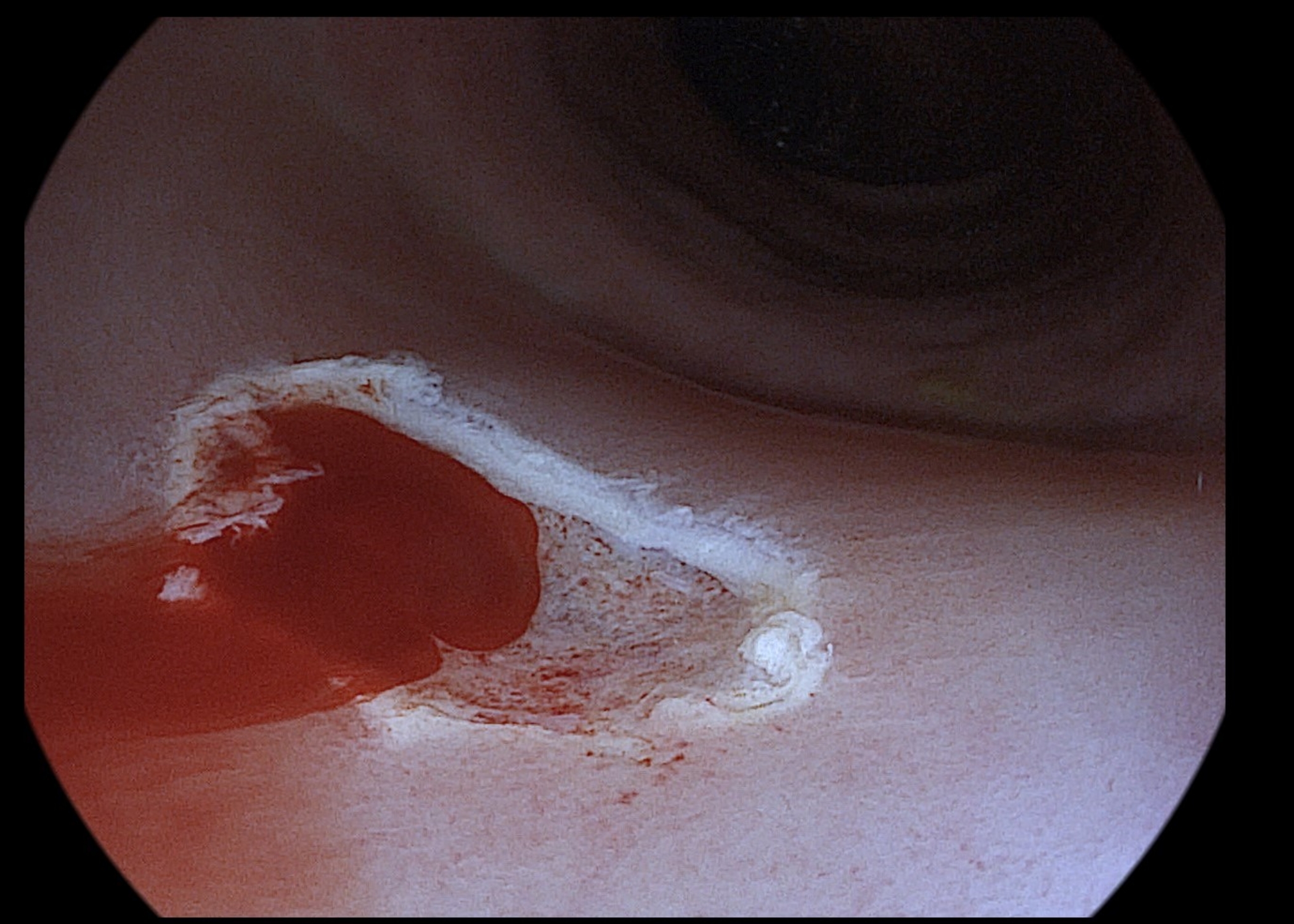
Image 6
How do I use PENTAX IMAGINA in my clinical endoscopy cases :
I use the IMAGINA system in every day clinical practice, especially in colorectal cancer screening program.
The high-quality image has resulted in an increased numbers of polyps detected.
Early rectal cancer treated with endoscopic full thickness resection
Patient History
53 years old men treated for arterial hypertension and dyslipidemia, with no CRC family history. Preventive colonoscopy after positive fecal immunochemical test. (FIT)
Endoscopic Findings
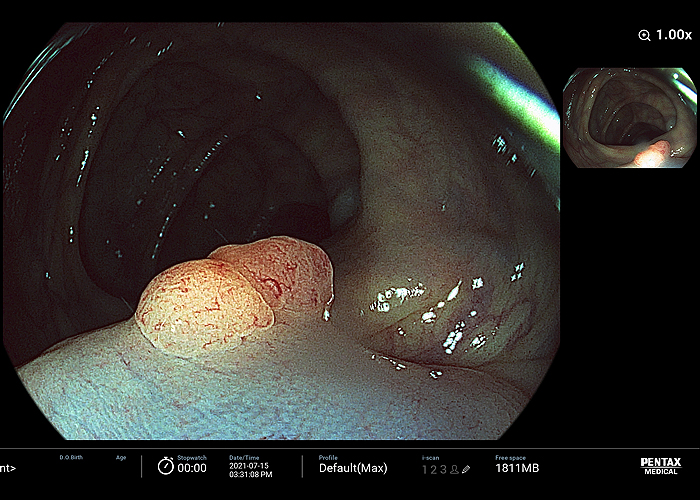
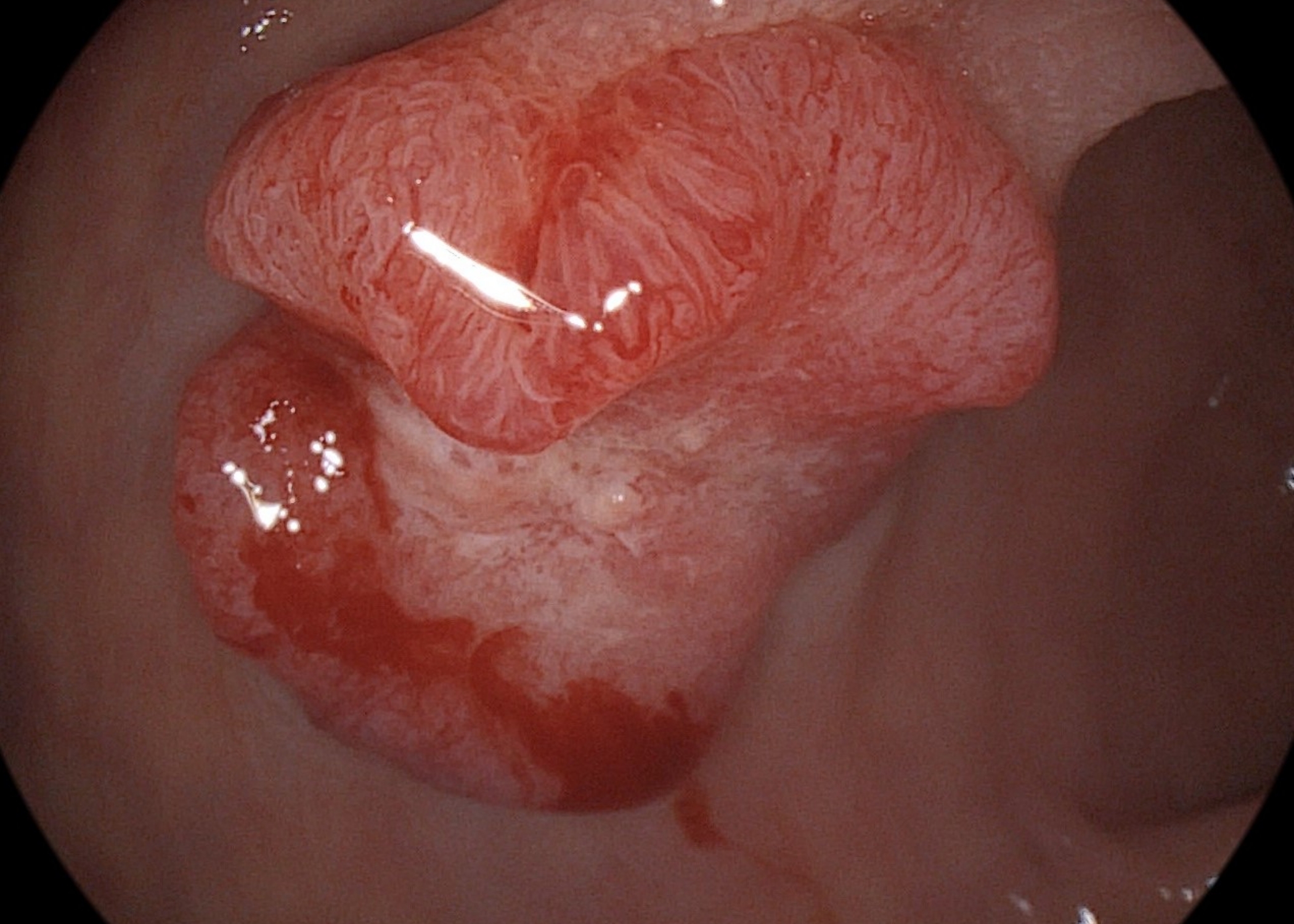
Sessile polyp in oral rectum (12 cm from anorectal line) with central depression, Paris classification 0-Is + 0-IIc, size 25 x 25 mm, macroscopically high suspicion of early cancer, according to HD-WLE (Image 1) and i-scan (Image 2)
Staging
Rectal ultrasound with submucosal infiltration without involvement of muscularis propria, staging T1N0. CT scan negative, MRI staging T2N0.
Endoscopic Treatment
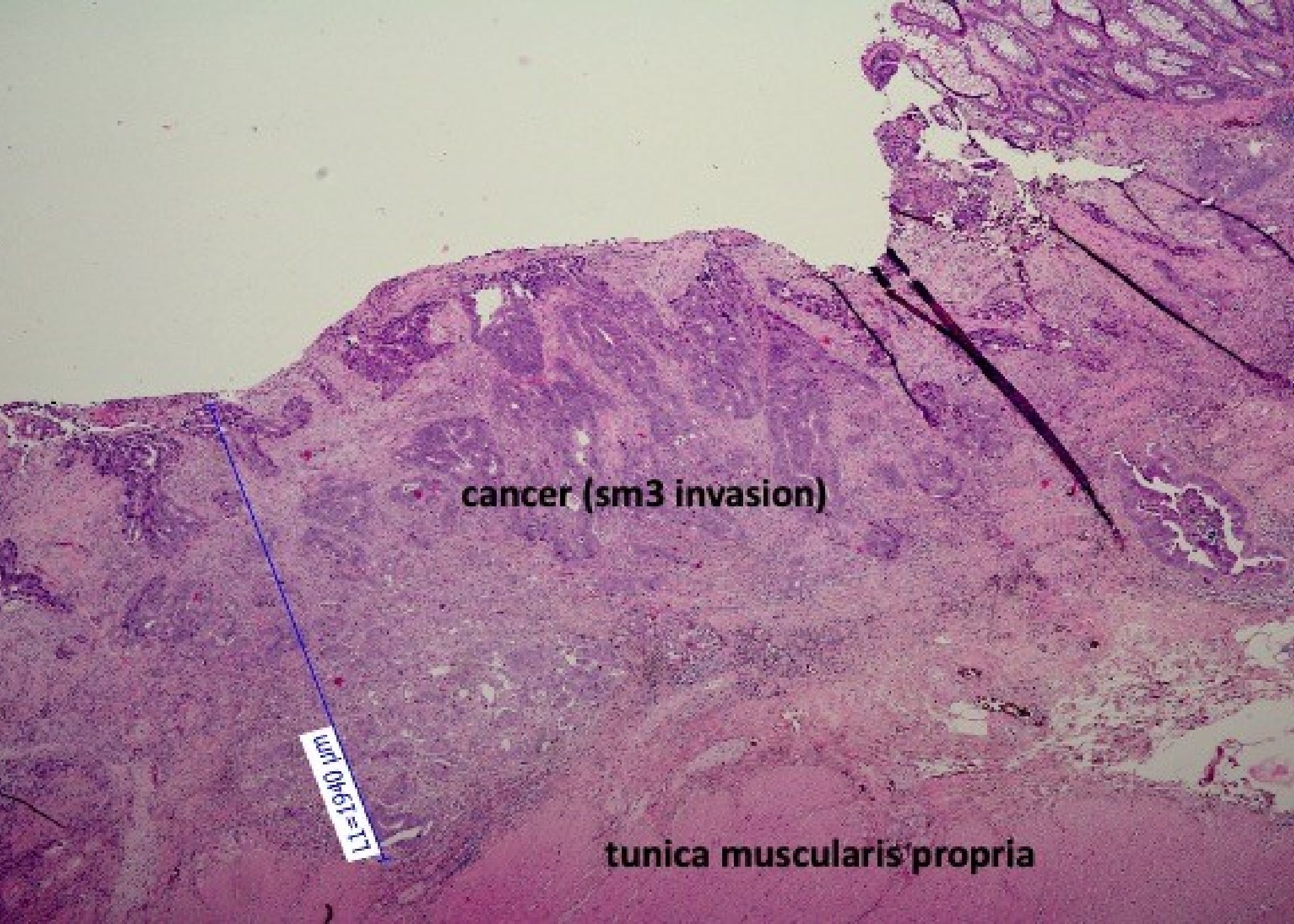
Lesion was completely removed by endoscopic full thickness resection (EFTR) Histopathology results: tubular adenocarcinoma, grade 1-2, pT1, sm3 (1900 um), LVI-, PNI-, R0 resection (2 mm), (Image 3)
Patient Outcome and Follow-ups
Patient denied subsequent surgical therapy. Close follow-up, rectoscopy in 6 months and colonoscopy and CT scan in 1 year. After 1 year all examination negative, scar in rectum intact, no metachronous lesions in colorectum, no metastasis.
Image 1
Image 2
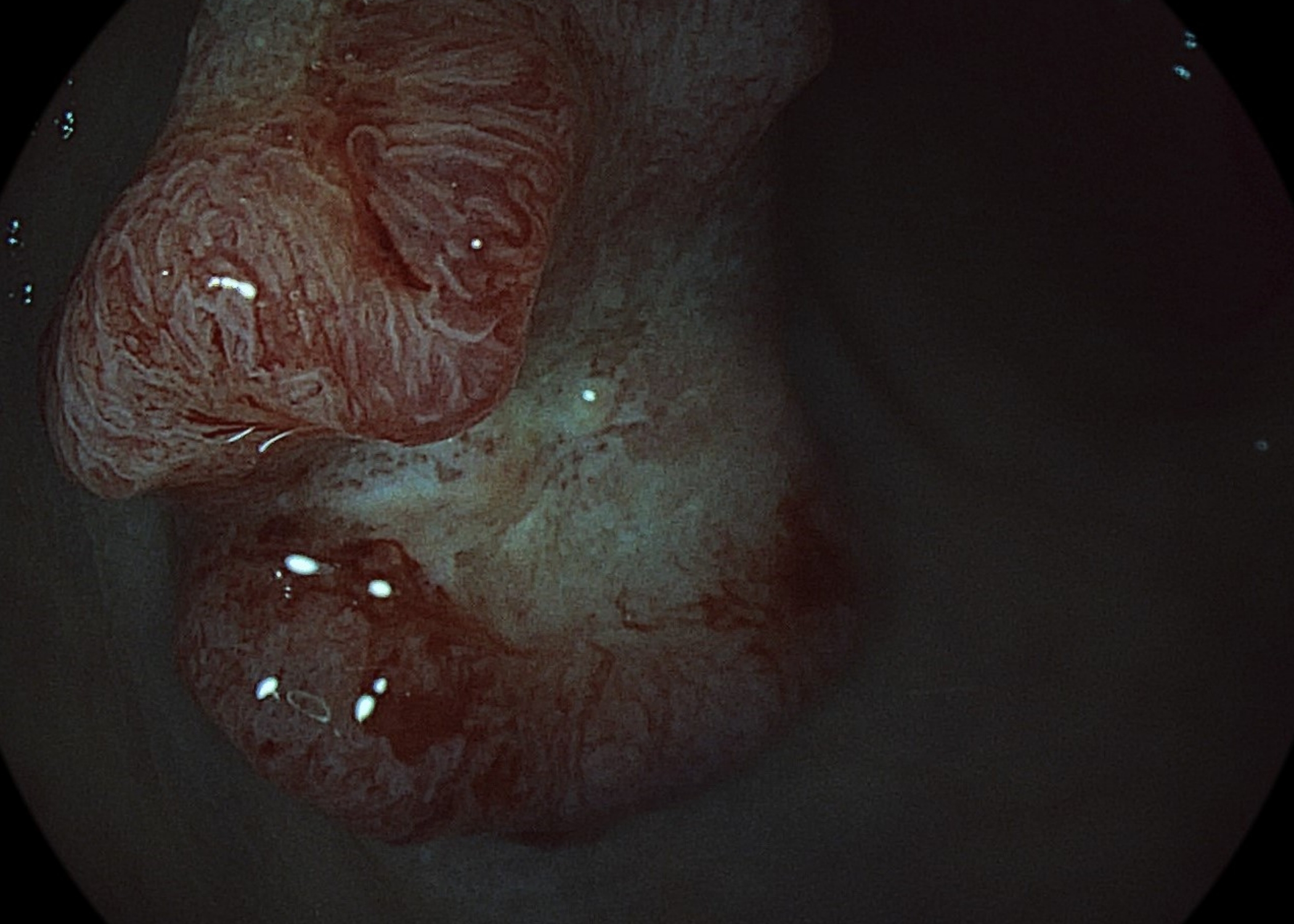
Image 3
COLON
>
CASE 1
CASE 2
CASE 3
How do I use
PENTAX IMAGINA
in my clinical endoscopy
cases :
“ I use PENTAX IMAGINA for colorectal cancer surveillance in patients with long-standing ulcerative colitis (UC).
Previously, I had performed surveillance using traditional random biopsies or pan-chromoendoscopy with targeted biopsies,
which required a lot of effort and time. Recently, however, I’m using image-enhanced endoscopy (virtual chromoendoscopy)
like NBI or i-scan which is more convenient.
Although still controversial, high definition-virtual chromoendoscopy is known to be comparable to dye-spraying chromoendoscopy in detecting neoplasia in UC.
I assume that combination of high-definition endoscopy with i-scan of PENTAX IMAGINA system can be useful for colorectal cancer surveillance in UC.“
Cascade Stomach
Patient History
A 51-year-old male patient with long-standing ulcerative colitis underwent surveillance colonoscopy for detection of dysplasia.
Endoscopic Findings
With HD-WLE, old cicatricial changes with whitish scars and numerous inflammatory polyps were observed throughout the entire colon distal to A-colon. There showed no active lesions. (image 1)
With HD + i-scan, an ovoid flat elevated lesion (6 mm) was detected in mid T-colon. The lesion showed brown and irregular. Surface. (image 2)
Another ovoid flat lesion (4 mm) was detected in proximal T-colon. (image 3)
i-scan helped to find dysplasia and demarcate the borders of the lesions.
Endoscopic Treatment
and Pathology Results
Two lesions were removed by endoscopic mucosal resection.
he final pathology was ‘tubular adenoma with low grade dysplasia’ in both lesions.
Patient Outcome and
Follow-ups
Two colitic neoplasia were detected and removed successfully by surveillance colonoscopy.
The patient recommended to have regular surveillance colonoscopy.
Image 1
Image 2
Image 3
Summary
How do I use
PENTAX IMAGINA
in my clinical endoscopy
cases :
“ I use PENTAX IMAGINA in my endoscopic procedures.
When an endoscopist performs a procedure, securing clean vision and smooth operation of endoscopy are essential factors. In this aspect, clear resolution and good maneuverability of PENTAX IMAGINA can be of great help to my successful procedure.”
Prophylactic Clip
Application for the
Prevention of
Postpolypectomy
Bleeding of Large
Pedunculated
Colonic Polyps
Patient History
A 46-year-old male patient was referred for a large pedunculated colon polyp.
Endoscopic Findings
With HD-WLE, a 15 mm sized pedunculated polyp was noted in the hepatic flexure. The length and width of stalk was 30 x 8 mm. (image 1)
The surface of the polyp head showed hyperemia and nodularity.
With HD + i-scan, vessels with variable caliber and irregular surface pattern were noted. (image 2)
i-scan helped to define the microvascular and surface patten of the lesion.
Endoscopic Treatment and Pathology Results
To prevent post-polypectomy bleeding, hemoclip was applied to the base of stalk before resection.
Then, hot snare polypectomy was performed. (image 3)
The final pathology was early colon cancer.
Adenocarcinoma, moderately differentiated, arising in sessile serrated adenoma with cytologic dysplasia
a) Size: adenoma 1.5 x 1.5 cm, carcinoma 0.7 x 0.7 cm
b) sm invasion = 300 ㎛ (Haggit level 1)
c) Tumor budding: absent
d) Resection margin involvement: absent
Image 1
Image 2
Image 3
Summary
How do I use
PENTAX IMAGINA
in my clinical endoscopy
cases :
“ I use PETAX IMAGINA for colorectal cancer (CRC) screening. Higher quality colonoscopic withdrawal techniques, such as
(1)examining the proximal sides of flexures, folds and valves, (2) cleaning and suctioning, (3) adequacy of distention, and
(4) adequacy of time spent viewing, are associated with lower adenoma missing rate.
I think that clean resolution and good maneuverability of PENTAX IMAGINA may help to improve the yield of CRC screening.”
Prophylactic Clip
Application for the
Prevention of
Postpolypectomy
Bleeding of Large
Pedunculated
Colonic Polyps
Detection of Sessile
Serrated Adenoma
in the Ascending
Colon
Patient History
A 60-year-old female patient underwent colonoscopy for bloating and constipation.
Endoscopic Findings
With HD-WLE, a subtle flat lesion was suspected in the distal A-colon.
After adjusting for air inflation, an ovoid flat elevated lesion was clearly observed. (image 1)
With HD + i-scan, the surface of lesion showed slightly lighter color than background mucosa and some dark dots, suggesting a hyperplastic or
sessile serrated polyp. (image 2)
i-scan helped to define the microvascular and surface pattern of the lesion.
Endoscopic Treatment and Pathology Results
Endoscopic mucosal resection was done. (image 3)
The final pathology was sessile serrated adenoma.
Sessile serrated adenoma without cytologic dysplasia.
1) size: 0.8x0.8cm
2) resected margin involvement: absent
Patient Outcome and Follow-ups
The procedure performed successfully without any event.
Image 1
Image 2
Image 3
Summary
COLON
>
How do I use
PENTAX IMAGINA
in my clinical endoscopy
cases :
“I use PENTAX IMAGINA in daily clinical endoscopy practice. One of our endoscopy purpose is surveillance after surgery or endoscopic resection of colorectal dysplasia or cancer. I frequently encounter metachronous polyps during this surveillance and the pathology provide exact diagnosis after resection of the polyp.
However, it is important to select exact candidates for colonoscopic resection to avoid unnecessary procedure.
I assume that PENTAX IMAGINA TE mode is useful in this aspect. JNET classification is useful tool in clinical decision.
Type 1 indicates a hyperplastic polyp or a sessile serrated adenoma/polyp.
Type 2A indicates low-grade dysplasia and includes tubular adenoma and tubulovillous adenoma.
Type 2B indicates high-grade dysplasia, intramucosal cancer, and superficial submucosal invasive cancer.
Type 3 indicates deep submucosal invasive cancer.
The PENTAX IMAGINA system have clear resolution and it can let me help to clear diagnosis. “
Endoscopic
Differentiation of
Colon Polyps
Patient History
The patient is a 61-year-old male who underwent sigmoid colon cancer surgery 2 years ago.
He is on adjuvant chemotherapy and colonoscopy surveillance was recently performed.
Endoscopic Findings
The colonoscopy revealed 8mm sized sessile polyp at transverse colon.
Endoscopic Treatment and Pathology Results
Endoscopic mucosal resection was done after submucosal injection and snaring.
No bleeding or perforation was noted after procedure. The final pathology was tubular adenoma, measuring 8mm in size.
Patient Outcome and Follow-ups
The patient will have another surveillance colonoscopy 2 or 3 year later.
Image 1,2 & 3
The i-scan SE shows sessile polyp with whitish surface mimicking sessile serrated polyp. However, the vascular and surface pattern was regular without white spots on i-scan TE image.
So, I can expect the pathology as a low-grade dysplasia based on JNET classification.
Summary
COLON
>
CASE 1
CASE 2
How do I use
PENTAX IMAGINA
in my clinical endoscopy
cases :
I use the IMAGINA system in every day clinical practice, especially in colorectal cancer screening program.
The high-quality image has resulted in an increased numbers of polyps detected.
Endoscopy mucosal resection of
traditional serrated lesion with high-grade dysplasia in sigmoid colon
Patient History
65 years old men with no CRC family history.
Preventive colonoscopy after positive fecal immunochemical test.
Endoscopic Findings
Sessile polyp in aboral sigmoid colon
(20 cm from anorectal line), Paris classification 0-Is, size 30 x 20 mm,
macroscopically adenomatous appearance according to the high-definition white light endoscopy
(HD-WLE, Image 1),
i-scan 1 (Image 2), i-scan 2 (Image 3),
i-scan 3 (Image 4)
Endoscopic treatment
Polyp was completely removed by endoscopic mucosal resection (EMR), after submucosal injection of saline solution with diluted Adrenaline.
Immediate bleeding from post-EMR site (Image 5) was stopped with snare tip coagulation,
haemoclips and nylon loop snare replacement(Image 6).
Endoscopic Treatment and Pathology Results
Traditional serrated lesion with high-grade
dysplasia, R0 resection.
Patient Outcome and Follow-ups
No sign of bleeding recurrence. Surveillance colonoscopy in 1 year negative with intact scar and no metachronous lesions in colorectum.
Image 1
Image 2
Image 3
Image 4
Image 5
Image 6
How do I use PENTAX
IMAGINA in my clinical
endoscopy cases :
I use the IMAGINA system in every day clinical practice, especially in colorectal cancer screening program. The high-quality image has resulted in an increased numbers of polyps detected.
Early rectal cancer treated with endoscopic full thickness resection
Patient History
53 years old men treated for arterial hypertension and dyslipidemia, with no CRC family history. Preventive colonoscopy after positive fecal immunochemical test. (FIT)
Endoscopic Findings
Sessile polyp in oral rectum (12 cm from anorectal line) with central depression, Paris classification 0-Is + 0-IIc, size 25 x 25 mm, macroscopically high suspicion of early cancer, according to HD-WLE (Image 1) and i-scan (Image 2)
Staging
Rectal ultrasound with submucosal infiltration without involvement of muscularis propria, staging T1N0. CT scan negative, MRI staging T2N0.
Endoscopic Treatment
Lesion was completely removed by endoscopic full thickness resection (EFTR)
Histopathology results: tubular adenocarcinoma, grade 1-2, pT1, sm3 (1900 um), LVI-, PNI-, R0 resection (2 mm), (Image 3)
Patient Outcome and Follow-ups
Patient denied subsequent surgical therapy. Close follow-up, rectoscopy in 6 months and colonoscopy and CT scan in 1 year.
After 1 year all examination negative, scar in rectum intact, no metachronous lesions in colorectum, no metastasis.
Image 1
Image 2
Image 3
PENTAX MEDICAL KOREA
11F, 42 Olympic-ro 35da-gil, Songpa-gu, Seoul, Korea 05510
Tel. +82-1544-9954Email. inquiryKorea@pentaxmedical.com
PENTAX MEDICAL KOREA 11F, 42 Olympic-ro 35da-gil, Songpa-gu, Seoul, Korea 05510 Tel. +82-1544-9954 Email. inquiryKorea@pentaxmedical.com
SUBMITTED
Thank you